Most recent guideline publication:
Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing: 2017 Update (October 2017)
Updates since publication:
January 2024 update (edited March 2024):
Recently, individual patients have been reported (PMID 38129972) to carry only one of the two SNPs in the HapB3 haplotype (i.e., c.1236G>A without c.1129-5923C>G), suggesting that the two variants are not in complete linkage disequilibrium. To address this, CPIC updated the allele definition and functionality tables to include the c.1129-5923C>G SNP separately as this is likely the causal variant leading to decreased function. CPIC also retained the HapB3 haplotype definition for cases where only the c.1236G>A variant is tested (e.g. whole exome sequencing). While CPIC recommends to directly test the causal SNP if possible, in cases where only c.1236G>A is tested or results are available for, it should be clearly stated in the test report that “decreased function” was inferred by detecting the exonic tag SNP, and disclose that in rare cases, the causal decreased function variant c.1129-5923C>G may not be present despite having this tag SNP. While there is no literature of a case that was negative for the tag SNP but positive for the intronic SNP (i.e., c.1129-5923C>G without c.1236G>A), the possibility still exists given the fact that the two SNPs are not in 100% LD. In such a case, testing for the tag SNP alone would result in a false negative.
A recent publication (PMID 37639651) reported evidence for a potentially reduced treatment effectiveness in DPYD c.1236G>A (HapB3) carriers receiving fluoropyrimidine dosing reduced by 25%. In the same patient group, also significantly increased toxicity was observed. The guideline authors have reviewed this paper and concluded that further studies need to be performed before potentially changing the dosing recommendation for this risk variant. It was noted that in this study, in the majority of patients receiving genotype-based dose reductions, no dose escalation was performed as is recommended in the CPIC guideline. Given this evidence for substantial interpatient variability among heterozygous carriers of a single decreased function variant (activity score 1.5), particular emphasis should be placed on dose titration after the initial dosing in this patient group. This guideline is in the process of being updated and these recommendations will be reviewed based on a complete evidence review.
February 2020 Update:
The DPYD allele functionality table and DPYD genotype-phenotype table have been updated (see the “change log” in each table for changes).
January 2020 Update:
The DPYD allele functionality table, DPYD frequency table, and DPYD genotype-phenotype table have been updated (see the “change log” in each table for changes).
November 2018 Update:
The current DPYD guideline recommends to reduce the dose of fluoropyrimidines by 25-50% (from the full standard dose) in DPYD Intermediate Metabolizers with an activity score of 1.5. At the time of the guideline publication, this dose range was recommended due to limited evidence for genotype-guided dosing of decreased function alleles/variants. However, a recent prospective study (PMID: 30348537) provides evidence to support a recommendation for a 50% dose reduction in heterozygous carriers of the decreased function variants c.2846A>T (rs67376798) or c.1129–5923C>G (rs75017182; HapB3 or its tagging SNP c.1236G>A; rs56038477). These data suggest that all Intermediate Metabolizers with an activity score of 1.5 should receive a 50% dose reduction. Therefore CPIC revises its recommendation such that all DPYD Intermediate Metabolizers should receive a 50% dose reduction from the full standard starting dose, whether the activity score is 1 or 1.5 followed by dose titration, based on clinical judgement and ideally therapeutic drug monitoring.
In addition, recent case reports from patients who are homozygous for c.2846A>T (activity score of 1) indicate that a dose reduction of more than 50% may be required in some carriers of this genotype. Therefore, in patients with an activity score of 1 due to a homozygous c.[2846A>T];[2846A>T] genotype, clinicians should be aware that a >50% reduction in starting dose might be warranted.
Tables provided in the main manuscript of the guideline:
| Table 1. Assignment of likely DPD phenotype based on DPYD genotype |
| Table 2. Recommended dosing of fluoropyrimidines by DPD phenotype |
Supplement to: Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing: 2017 Update (October 2017)
Tables included in the supplement or referenced in the guidelinea:
| Supplemental Table S1. Evidence linking DPYD genotype with DPD phenotype and dihydropyrimidine toxicity |
| DPYD allele definition table |
| DPYD allele functionality table |
| DPYD frequency table |
| DPYD genotype-phenotype table |
| Gene resource mapping |
| Drug resource mapping |
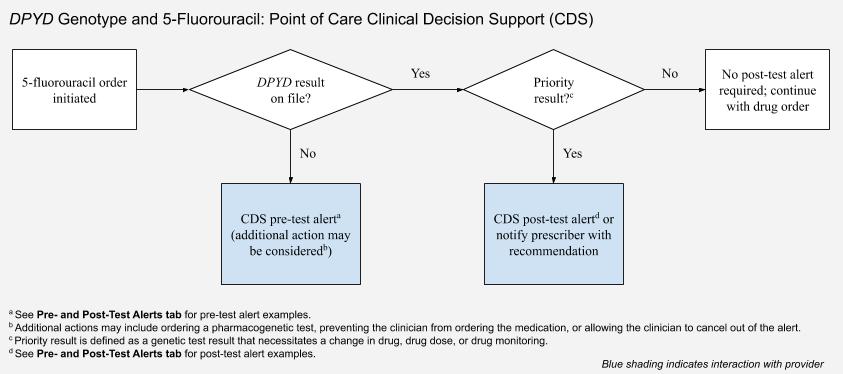
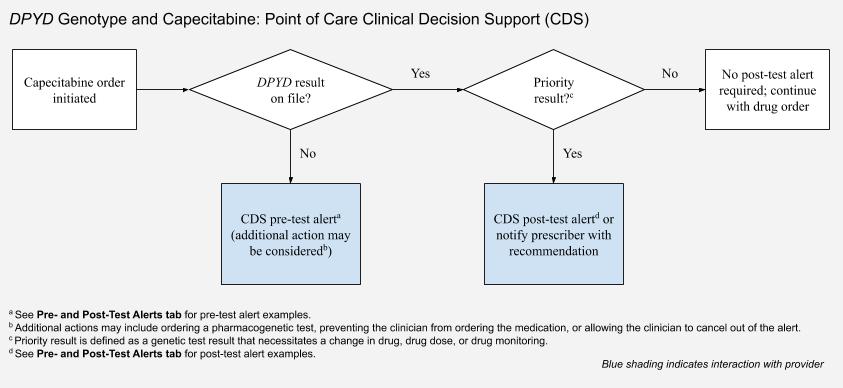
| Clinical decision supportb: |
{kind=link}
{kind=link}
{kind=link}
aSome of the tables included in the guideline may have been updated online, particularly to reflect newly described or newly characterized alleles. These include the gene-specific information tables (https://www.pharmgkb.org/page/pgxGeneRef) that support CPIC guidelines by providing information regarding star (*) allele definitions, allele function, allele frequency by major ethnic groups, translations of diplotype to phenotype, and gene resource mappings.
bThese resources support the adoption of CPIC guidelines into the electronic health record with clinical decision support and provide information that clinical implementers find helpful.
Original guideline publication (December 2013):
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing (December 2013)
- 2013 supplement
- May 2014: The CPIC authors recommend that the DPYD*4, *5, *6 and *9A alleles be categorized as “normal” activity, in part based upon the recent publication Comparative Functional Analysis of DPYD Variants of Potential Clinical Relevance to Dihydropyrimidine Dehydrogenase Activity. (Please note this update was incorporated into the 2017 update).